

Variants are monitored by sequencing as part of the national SARS-CoV-2 sequencing program.
To enable monitoring of these variants almost in "real time", without needing to wait for sequencing results, the HUG virology laboratory regularly carried out additional PCR tests on positive samples, which allowed for to determination of the variant.
This strategy made it possible to closely monitor the succession of different variants over time, offering a rapid and precise overview of the the epidemiology, and also had direct therapeutic consequences for the choice of certain treatments (the monoclonal antibodies used in the prevention of progression against severe disease or in patients hospitalized with pneumonia).
Monitoring of variants by searching for specific mutations by PCR
Thanks to additional PCRs carried out on a selection of positive samples with suitable viral loads (Ct value < 32), monitoring the frequency of the N501Y mutation made it possible to highlight the arrival of the first variant of interest, the Alpha variant, from December 2020. In the summer of 2021, Delta quickly replaced this Alpha variant in the space of a few weeks. This evolution could be followed by the search for the L452R mutation, carried out by our laboratory. Sequencing was quickly able to confirm this data.
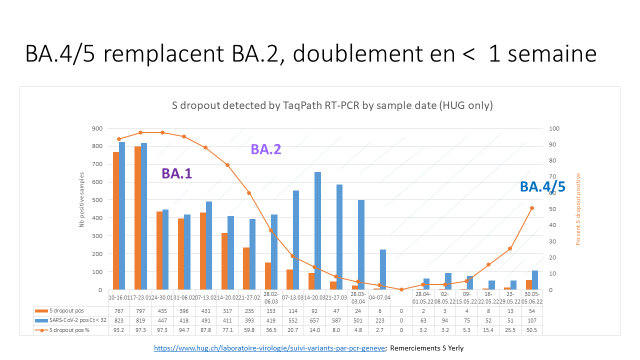
S-gene dropout PCR monitoring of different variants
Additionally, since the start of the pandemic, a deletion that causes a failure to amplify the S-gene target, referred to as "S-gene dropout", in a PCR test (TaqPath RT-PCR) has been useful for tracking the spread of certain variants. This deletion was found to alternate between being present or absent in the successive variants, which made it possible to discriminate between them over time.
This method was useful for monitoring the appearance of Omicron BA.2.86, then the sequential replacements of BA.1 by BA.2, BA.2 by BA.5, BA.5 by XBB and XBB by JN.1, as can be seen below (graphs under +INFOS).
R346T mutation follow-up
The R:346T mutation in the BA.5 background has been described as an escape mutation to the monoclonal antibody cilgavimab, which is a key component of Evusheld®. Initially, screening for this mutation by PCR (TIB Molbiol) allowed for rapid determination of whether Evusheld® would likely be useful in treating the infection. R346T rapidly became present in nearly all the circulating variants, and screening for this mutation was stopped in January 2023. This mutation dissappeared again as JN.1 replaced the previous variants.
Recently (March 2024), this mutaiton has been appearing in JN.1 sublineages in increasing in frequency, and the PCR test is ready to be reimplemented if deemed neccessary.
{kind=link}